Introduction
Physiotherapy in Cambridge, Galt, and Preston for Achilles Pain

Welcome to The Cambridge Physiotherapy's patient resource about Achilles Tendon Problems.
Problems that affect the Achilles tendon include tendonitis, tendinopathy, tendocalcaneal bursitis, and tendonosis. Each of these conditions will be described and explained. These problems affect athletes most often, especially runners, basketball players, and anyone engaged in jumping sports. They are also common among both active and sedentary (inactive) middle-aged adults. These problems cause pain at the back of the calf. Severe cases may result in a rupture of the Achilles tendon.
This guide will help you understand:
- where the Achilles tendon is located
- what kinds of Achilles tendon problems there are
- how an injured Achilles tendon causes problems
- what treatment options are available
#testimonialslist|kind:all|display:slider|orderby:type|filter_utags_names:Foot therapy|limit:15|heading:Hear from some of our *Foot Therapy* patients#
Anatomy
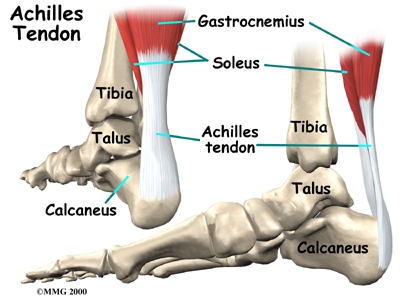
Where is the Achilles tendon, and what does it do?
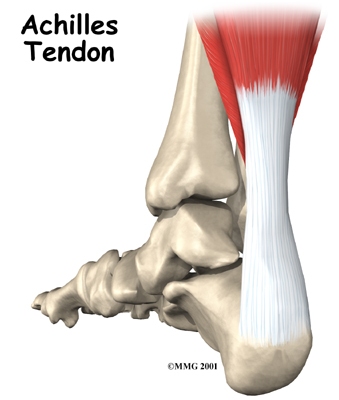
The Achilles tendon is a strong, fibrous band that connects the calf muscle to the heel. The calf is actually formed by two muscles, the underlying soleus and the thick outer gastrocnemius. Together, they form the .
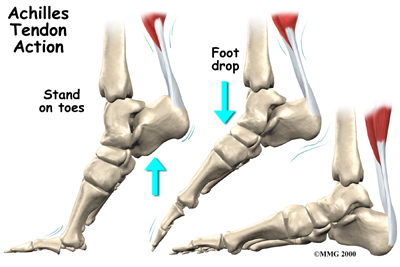
When they contract, they pull on the Achilles tendon, causing your foot to point down and helping you rise on your toes. This helps when you sprint, jump, or climb. Several different problems can occur that affect the Achilles tendon, some rather minor and some quite severe.
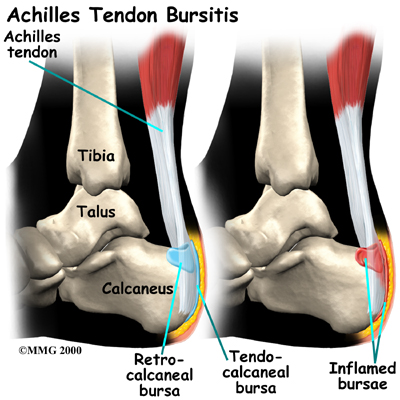
A bursa is a fluid-filled sac designed to limit friction between rubbing parts. These sacs, or bursae, are found in many places in the body. When a bursa becomes inflamed, the condition is called bursitis. is an inflammation in the bursa behind the heel bone. This bursa normally limits friction where the thick fibrous Achilles tendon that runs down the back of the calf glides up and down behind the heel.
Achilles Tendonitis
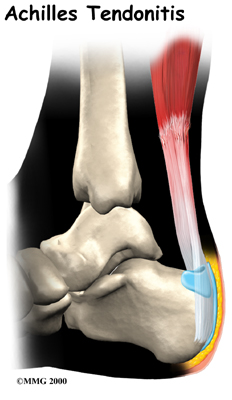
A violent strain can cause trauma to the calf muscles or the Achilles tendon. Sometimes this is referred to as tendonitis. This injury can happen during a strong contraction of the muscle, as when running or sprinting. Landing on the ground after a jump can force the foot upward, also causing injury. The strain can affect different portions of the muscles or tendon. For instance, the strain may 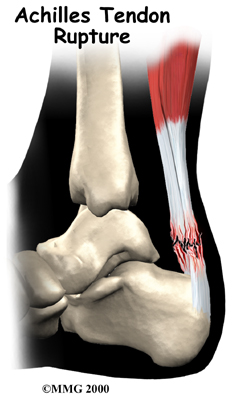 occur in the center of the muscle. Or it may happen where the muscles join the Achilles tendon (called the musculotendinous junction).
occur in the center of the muscle. Or it may happen where the muscles join the Achilles tendon (called the musculotendinous junction).
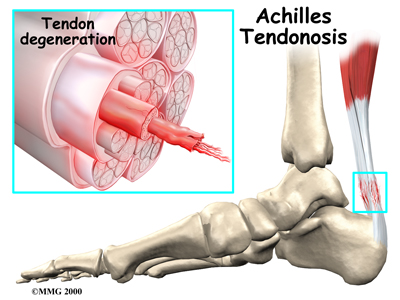
Achilles Tendinopathy/Tendonosis
Chronic overuse may contribute to changes in the Achilles tendon as well, leading to degeneration and thickening of the tendon. Studies show there is no sign of inflammation with overuse injuries of tendons. Most experts now refer to this condition as tendinopathy or tendonosis instead of tendonitis.
Achilles Tendon Rupture
In severe cases, the force of a violent strain may even . The classic example is a middle-aged tennis player or weekend warrior who places too much stress on the tendon and experiences a tearing of the tendon. In some instances, the rupture may be preceded by a period of tendonitis, which renders the tendon weaker than normal.
Related Document: client_company*'s Patient's Guide to Foot Anatomy
Causes
How do these problems develop?
It’s not entirely clear why these problems develop in some people but not in others. Changes in the normal alignment of the foot and leg may be part of the problem. Anyone with one leg shorter than the other is at increased risk of Achilles tendon problems.
 For the athlete, sudden increases in training may be a key factor. Runners may add on miles or engage in excessive hill training while other athletes increase training intensity. Other risk factors include obesity, diabetes (or other endocrine disorders), aging, exposure to steroids, and taking fluoroquinolones (antibiotics).
For the athlete, sudden increases in training may be a key factor. Runners may add on miles or engage in excessive hill training while other athletes increase training intensity. Other risk factors include obesity, diabetes (or other endocrine disorders), aging, exposure to steroids, and taking fluoroquinolones (antibiotics).
Problems with the Achilles tendon seem to occur in different ways. Initially, irritation of the outer covering of the tendon, called the paratenon, causes paratendonitis. Paratendonitis is simply inflammation around the tendon. Inflammation of the tendocalcaneal bursa (described above) may also be present with paratendonitis. Either of these conditions may be due to repeated overuse or ill-fitting shoes that rub on the tendon or bursa.
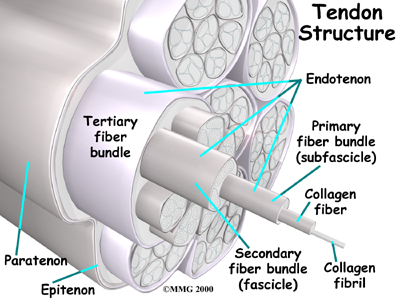
As we age, our tendons can degenerate. Degeneration means that wear and tear occurs in the tendon over time and leads to a situation where the tendon is weaker than normal. Degeneration in a tendon usually shows up as a loss of the normal arrangement of the fibers of the tendon. Tendons are made up of strands of a material called . (Think of a tendon as similar to a nylon rope and the strands of collagen as the nylon strands.)
 Some of the individual strands of the tendon become jumbled due to the , other fibers break, and the tendon loses strength.
Some of the individual strands of the tendon become jumbled due to the , other fibers break, and the tendon loses strength.
The healing process in the tendon causes the tendon to become thickened as scar tissue tries to repair the tendon. This process can continue to the extent that a nodule forms within the tendon. This degenerative condition without inflammation is called tendonosis. The area of tendonosis in the tendon is weaker than normal tendon. Tiny tears in the tissue around the tendon occur with overuse. The weakened, degenerative tendon sets the stage for the possibility of actual rupture of the Achilles tendon.
Symptoms
What do these conditions feel like?
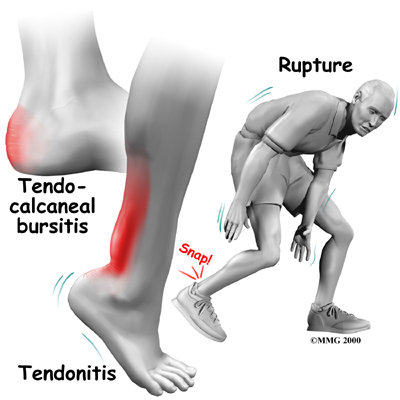
Tendocalcaneal bursitis usually begins with pain and irritation at the back of the heel. There may be visible redness and swelling in the area. The back of the shoe may further irritate the condition, making it difficult to tolerate shoe wear.
Achilles tendonitis usually occurs further up the leg, just above the heel bone itself. The Achilles tendon in this area may be noticeably thickened and tender to the touch. Pain is present with walking, especially when pushing off on the toes.
An Achilles tendon rupture is usually an unmistakable event. Some bystanders may report actually hearing the snap, and the victim of a rupture usually describes a sensation similar to being violently kicked in the calf. Following rupture the calf may swell, and the injured person usually can't rise on his toes.
Diagnosis
How do health care providers identify the problem?
Diagnosis of Achilles tendon problems is almost always made through clinical history and physical examination. The physical examination is used to determine specifically where your leg hurts.
When you visit The Cambridge Physiotherapy, our physiotherapist may perform some simple tests if a rupture is suspected. Your therapist may move your ankle in different positions and ask you to hold your foot against applied pressure. Palpation (feeling for any abnormalities in the tendon) and muscle function tests may also be included. By stretching the calf muscles and feeling where these muscles attach onto the Achilles tendon, we can begin to locate the problem area.
Some patients may be referred to a doctor for further diagnosis. Once your diagnostic examination is complete, the physiotherapists at The Cambridge Physiotherapy have treatment options that will help speed your recovery, so that you can more quickly return to your active lifestyle.
Our Treatment
Non-surgical Rehabilitation
When you begin physiotherapy at The Cambridge Physiotherapy, the rehabilitation program that our physiotherapist prescribes will depend on the specific type of problem (tendonitis or tendinopathy/tendonosis/tendon rupture) present.
Tendonitis/Tendinopathy
In the past, nonsurgical treatment for tendocalcaneal bursitis and Achilles tendonitis started with a combination of rest, ice, and anti-inflammatory medications prescribed by your doctor.
Since it is now recognized that many tendon problems occur without inflammation, the use of anti-inflammatories and ice have come into question. In the case of true inflammation, the overuse of these modalities may prevent a normal, healing inflammatory process. Preventing inflammation needed to clean up cellular debris in the injured area may lead to delayed or incomplete healing. The result may be future chronic problems of tendonosis and/or tendinopathy.
Many experts suggest that when there is any doubt about inflammation, treatment should proceed as if there are no inflammatory cells present. Our approach would then focus on pain relief and restoring proper motion and weight-bearing so you can return to your usual activities.
If there is an inflammatory process, then the condition should respond fairly quickly to drug and antiinflammatory interventions. Limiting, but not eliminating, inflammation is the new goal.
Our physiotherapists know when and how to apply cold modalities to reduce swelling and pain, while still allowing the healing inflammatory process. We may also apply treatments such as ultrasound, moist heat, and massage are used to control pain and inflammation. As pain eases, we will progresses your treatment to include stretching and strengthening exercises.
Tendonosis
If the problem is one of tendon tissue degeneration, healing and recovery may take longer. This type of injury will not respond to treatment designed to reduce inflammation. Correct treatment of tendonosis involves fostering new collagen tissue growth and improving the strength of the tendon. Rehabilitation following rupture of the tendon is quite different and is described later.
An acute injury needs rest. We recommend that initially, you limit activities that require walking on the sore leg. Although the time required for rehabilitation varies among patients, in cases of Achilles tendinopathy, or when a partial tendon tear is being treated without surgery, patients may require two to three months of physiotherapy.
Your physiotherapist may recommend that a small (one-quarter inch) heel lift be placed in your shoe to minimize stress by putting slack in the calf muscle and Achilles tendon. A similar sized lift will also be placed in the other shoe to keep everything aligned.
Injured tendons shorten and need to be stretched. Only gentle stretches of the calf muscles and Achilles tendon are used at first. As the tendon heals and pain eases, more aggressive stretches are given. Our therapist may also use ultrasound and massage to help the tendon heal.
As your condition improves, exercises to strengthen the calf muscles begin. Strengthening starts gradually using isometrics, exercises that work the muscles but protect the healing area. Eventually, specialized strengthening exercises, called eccentrics, are used, working the calf muscle while it lengthens.
The physiotherapy provided by The Cambridge Physiotherapy enables patients to gradually return to normal activities. We have specialized programs to guide athletes in rehabilitation that is specific to their type of sport.
Tendon Rupture
Nonsurgical treatment for an Achilles tendon rupture is somewhat controversial. It is clear that treatment with a cast will allow the vast majority of tendon ruptures to heal, but the incidence of rerupture is increased in those patients treated with casting for eight weeks when compared with those undergoing surgery. In addition, the strength of the healed tendon is significantly less in patients who choose cast treatment. For these reasons, many orthopedists feel that Achilles tendon ruptures in younger active patients should be surgically repaired.
Nonsurgical treatment might be considered for the aging adult who has an inactive lifestyle. This allows the patient to heal while avoiding the potential complications of surgery. The patient's foot and ankle are placed in a cast for aprroximately eight weeks. Casting the leg with the foot pointing downward brings the torn ends of the Achilles tendon together and holds them until scar tissue joins the damaged ends. During this time, your physiotherapist will instruct you in safe and proper crutch utilization. After your cast is removed, our physiotherapist can have your fitted with a large heel lift to wear for apprximately another six to eight weeks after the cast is taken off.
Post-surgical Rehabilitation
Although the time required for recovery is different for each individual, patients are typically placed in a cast, brace or splint for six to eight weeks after surgery to protect the repair and the skin incision. Your physiotherapist will help you learn to properly use crutches to keep from putting weight onto your foot too soon after surgery.
Devices used to immobilize the leg can cause joint stiffness, muscle wasting (atrophy), and blood clots. To avoid these problems, our therapist will have you start doing motion exercises very soon after surgery. Patients typically wear a splint or brace that can easily be removed to do the exercises throughout the day.
In this early-motion approach, you begin our physiotherapy program within the first few days after surgery. Your physiotherapist in Cambridge, Galt, and Preston may initially use ice, massage, and whirlpool treatments to limit (but not completely prevent) swelling and pain. Massage and ultrasound help heal and strengthen the tendon.
Our physiotherapy treatments eventually progress to include more advanced mobility and strengthening exercises, some of which may be done in a pool. The buoyancy of the water helps people walk and exercise safely without putting too much tension on the healing tendon. The splint is worn while walking usually for six to eight weeks after surgery.
As your symptoms ease and your strength improves, our physiotherapist will guide you through advancing stages of exercise. Athletes often begin running, cutting, and jumping drills by the fourth month after surgery, and although recovery time is different for each paitent, are usually able to get back to their sport by six full months after surgery.
Our goal is to help you keep your pain and swelling under control, improve your range of motion and strength, and ensure you regain a normal walking pattern. When your recovery is well under way, regular visits to the The Cambridge Physiotherapy will end. Although we will continue to be a resource, you will be in charge of doing your exercises as part of an ongoing home program.
The Cambridge Physiotherapy provides services for physiotherapy in Cambridge, Galt, and Preston.
Surgery
Surgical treatment for Achilles tendonitis is not usually necessary for most patients. Surgery options range from a tenotomy (a simple release of the tendon) to a more involved, open approach of repair.
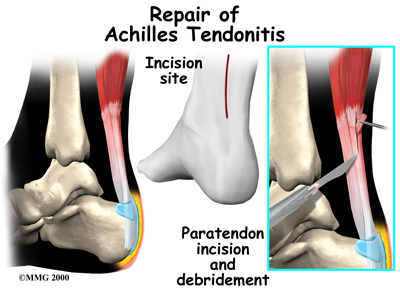
In some cases of persistent tendonitis and tendonosis a procedure called debridement of the Achilles tendon may be suggested to help treat the problem.
This procedure is usually done through an incision on the back of the ankle near the Achilles tendon. The tendon is identified, and any inflamed paratenon tissue (the covering of the tendon) is removed. The tendon is then split, and the degenerative portion of the tendon is removed. The split tendon is then repaired and allowed to heal. It is unclear why, but removing the degenerative portion of the tendon seems to stimulate repair of the tendon to a more normal state.
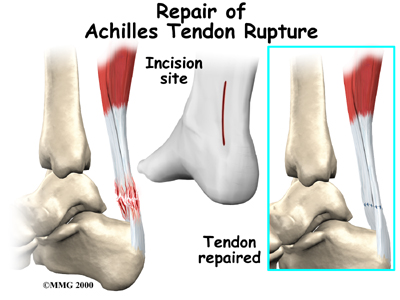
Surgery may also be suggested if you have a ruptured Achilles tendon. Reattaching the two ends of the tendon repairs the torn Achilles tendon. This procedure is usually done through an incision on the back of the ankle near the Achilles tendon. Numerous procedures have been developed to repair the tendon, but most involve sewing the two ends of the tendon together in some fashion. Some repair techniques have been developed to minimize the size of the incision.
In the past, the complications of surgical repair of the Achilles tendon made surgeons think twice before suggesting surgery. The complications arose because the skin where the incision must be made is thin and has a poor blood supply. This can lead to an increase in the chance of the wound not healing and infection setting in. Now that this is better recognized, the complication rate is lower and surgery is recommended more often.
Portions of this document copyright MMG, LLC.









