Introduction
Physiotherapy in Cambridge, Galt, and Preston for Knee
Welcome to The Cambridge Physiotherapy's patient resource about Quadriceps Tendonitis.
Alignment or overuse problems of the knee structures can lead to strain, irritation, and/or injury of the quadriceps muscle and tendon. This produces pain, weakness, and swelling of the knee joint.
These problems can affect people of all ages but the majority of patients with overuse injuries of the knee (and specifically quadriceps tendonitis) are involved in soccer, volleyball, or running activities.
This guide will help you understand:
- how the problem develops
- how doctors diagnose the condition
- what treatment options are available
#testimonialslist|kind:all|display:slider|orderby:type|filter_utags_names:Knee Pain|limit:15|heading:Hear from some of our patients who we treated for *Knee Pain*#
Anatomy
What is the quadriceps muscle/tendon, and what does it do?
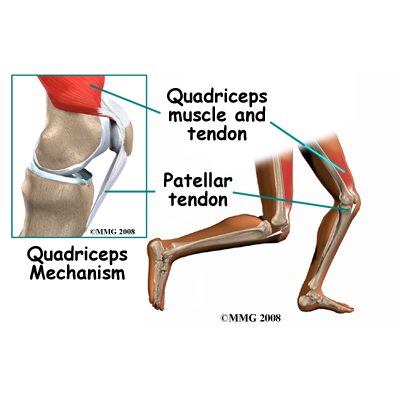
The patella (kneecap) is the moveable bone on the front of the knee. This unique bone is wrapped inside a tendon that connects the large muscles on the front of the thigh, the quadriceps muscles, to the lower leg bone.
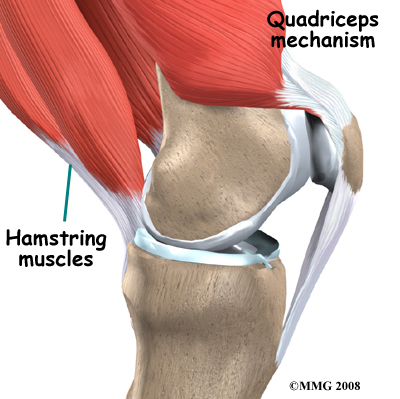
The large quadriceps muscle ends in a tendon that inserts into the tibial tubercle, a bony bump at the top of the tibia (shin bone) just below the patella. The tendon together with the patella is called the quadriceps mechanism. Though we think of it as a single device, the quadriceps mechanism has two separate tendons, the quadriceps tendon on top of the patella and the patellar tendon below the patella.
Tightening up the quadriceps muscles places a pull on the tendons of the quadriceps mechanism. This action causes the knee to straighten. The patella acts like a fulcrum to increase the force of the quadriceps muscles.
The long bones of the femur and the tibia act as level arms, placing force or load on the knee joint and surrounding soft tissues. The amount of load can be quite significant. For example, the joint reaction forces of the lower extremity (including the knee) are two to three times the body weight during walking and up to five times the body weight when running.
Related Document: The Cambridge Physiotherapy's Guide to Knee Anatomy
Knee Anatomy Introduction
Causes
How does this problem develop?
Quadriceps tendonitis occurs most often as a result of stresses placed on the supporting structures of the knee. Running, jumping, and quick starts and stops contribute to this condition. Overuse injuries from sports activities is the most common cause but anyone can be affected, even those who do not participate in sports or recreational activities.
There are extrinsic (outside) factors that are linked with overuse tendon injuries of the knee. These include inappropriate footwear, training errors (frequency, intensity, duration), and surface or ground (hard surface, cement) being used for the sport or event (such as running). Training errors are summed up by the rule of toos. This refers to training too much, too far, too fast, or too long. Advancing the training schedule forward too quickly is a major cause of quadriceps tendonitis.
 Intrinsic (internal) factors such as age, flexibility, and joint laxity are also important. Mal-alignment of the foot, ankle, and leg can play a key role in tendonitis. Flat foot position, tracking abnormalities of the patella, rotation of the tibia, and a leg length difference can create increased and often uneven load on the quadriceps mechanism. Any muscle imbalance of the lower extremity (from the hip down to the toes) can impact the quadriceps muscle and affect the joint. Individuals who are overweight may have added issues with load and muscle imbalance leading to quadriceps tendonitis.
Intrinsic (internal) factors such as age, flexibility, and joint laxity are also important. Mal-alignment of the foot, ankle, and leg can play a key role in tendonitis. Flat foot position, tracking abnormalities of the patella, rotation of the tibia, and a leg length difference can create increased and often uneven load on the quadriceps mechanism. Any muscle imbalance of the lower extremity (from the hip down to the toes) can impact the quadriceps muscle and affect the joint. Individuals who are overweight may have added issues with load and muscle imbalance leading to quadriceps tendonitis.
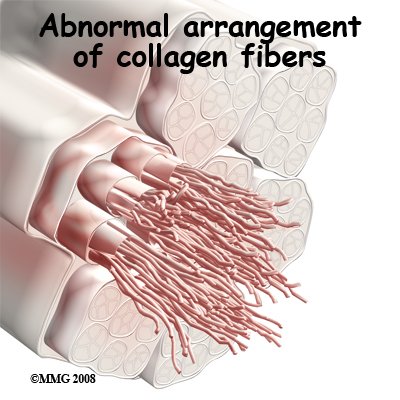
Strength of the patellar tendon is in direct proportion to the number, size, and orientation of the that make up the tendon. Overuse is simply a mismatch between load or stress on the tendon and the ability of that tendon to distribute the force. If the forces placed on the tendon are greater than the strength of the structure, then injury can occur. Repeated microtrauma at the muscle tendon junction may overcome the tendon's ability to heal itself. Tissue breakdown occurs triggering an inflammatory response that leads to tendonitis and even partial tears.
Chronic quadriceps tendonitis is really a problem called tendonosis. Inflammation is not present. Instead, degeneration and/or scarring of the tendon has developed. Chronic tendon injuries are much more common in older athletes (30 to 50 years old).
Symptoms
What does the condition feel like?
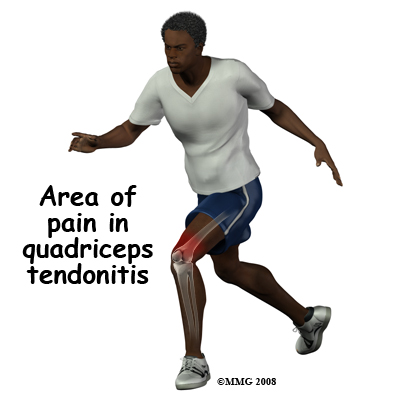
Pain from quadriceps tendonitis is felt in the area at the bottom of the thigh, just above the patella. The pain is most noticeable when you move your knee. The more you move your knee, the more tenderness develops in the area of the tendon attachment above the kneecap.
There may be swelling in and around the quadriceps tendon. It may be tender or very sensitive to touch. You may feel a sense of warmth or burning pain. The pain can be mild or in some cases the pain can be severe enough to keep the runner from running or other athletes from participating in their sport. Stiffness of the knee is common when you first get up in the morning (or after a long period of rest or inactivity), and during and after exercise.
Diagnosis
How is quadriceps tendonitis diagnosed?
When you first visit The Cambridge Physiotherapy, diagnosis begins with a complete history of your knee problem followed by an examination of the knee, including the patella. There is usually tenderness with palpation of the inflamed tissues at the insertion of the tendon into the bone. We will assess you knee for range of motion, strength, flexibility and joint stability.
Our physiotherapists will look for intrinsic and extrinsic factors affecting the knee (especially sudden changes in training habits). Potential problems with lower extremity alignment are identified. We will also check to see if the quadriceps tendon is partially torn or ruptured. Weakness of the extensor mechanism is a sign of such an injury.
You may be referred to a physician if a more serious pathology is suspected or your symptoms are not responding to physiotherapy.
Our Treatment
What treatment options are available?
Prevention of future injuries through patient education is a key component of our treatment program. This is true whether conservative care or surgical intervention is required. Modification of intrinsic and extrinsic risk factors is essential.
Non-surgical Rehabilitation
At The Cambridge Physiotherapy, the initial treatment for acute quadriceps tendonitis begins by decreasing the inflammation in the knee. Our physiotherapist may suggest relative rest and anti-inflammatory medications, such as aspirin or ibuprofen, especially when the problem is due to overuse. Acetaminophen (Tylenol®) may be used for pain control if you can't take anti-inflammatory medications for any reason.
Relative rest is a term used to describe a process of rest-to-recovery based on the severity of symptoms. If you have pain at rest, strict rest is required and possibly a short time of immobilization in a splint or brace. When pain is no longer present at rest, then a gradual increase in activity is allowed so long as the resting pain doesn't come back.
Physiotherapy can help in the early stages by decreasing pain and inflammation. When you begin your physiotherapy program, we may initially use ice massage, electrical stimulation, and ultrasound to limit pain and control (but not completely prevent) swelling. Some amount of inflammatory response is needed for a good healing response.
Our physiotherapist will prescribe stretching and strengthening exercises to correct any muscle imbalances. Eccentric muscle strength training helps prevent and treat injuries that occur when high stresses are placed on the tendon during closed kinetic chain activities. Eccentric contractions occur as the contracted muscle lengthens. Closed kinetic chain activities means the foot is planted on the floor as the knee bends or straightens.
We often recommend flexibility exercises designed for the thigh and calf muscles. Specific exercises are used to maximize control and strength of the quadriceps muscles. We will show you how to ease back into jumping or running sports using good training techniques. Off-season strength training of the legs, and particularly the quadriceps muscles is advised.
Bracing or taping the patella can help you do exercises and activities with less pain. Most braces for patellofemoral problems are made of soft fabric, such as cloth or neoprene. You slide them onto your knee like a sleeve. A small buttress pads the side of the patella to keep it lined up within the groove of the femur. An alternative to bracing is to tape the patella in place. Our physiotherapist can apply and adjust the tape over the knee to help realign the patella. The idea is that by bracing or taping the knee, the patella stays in better alignment within the femoral groove. This in turn is thought to improve the pull of the quadriceps muscle so that the patella stays lined up in the groove. Patients report less pain and improved function with these forms of treatment.
Our physiotherapists may also recommend special shoe inserts, called orthotics, to improve knee alignment and function of the patella. Proper footwear for your sport is important.
Coaches, trainers, and physiotherapists can work together to design a training program that allows you to continue training without irritating the tendon and surrounding tissues. Remember to warm up and stretch before exercise. Some experts recommend a cool down and stretching after exercise as well. Know your limits and don't overdo it.
Use ice after activity if indicated by pain or swelling. Icing should be limited to no more than 20 minutes to avoid reflex vasodilation (increased circulation to the area to rewarm it causing further swelling). Heat may be used in cases of chronic tendinosis to stimulate blood circulation and promote tissue healing.
Whenever you have to miss exercising for any reason or when training for a specific event, adjust your training schedule accordingly. Avoid the "too" training errors mentioned earlier.
Quadriceps tendonitis is usually self-limiting. That means the condition will resolve with rest, activity modification, and physiotherapy. Recurrence of the problem is common for patients who fail to let the quadriceps tendon recover fully before resuming training or other aggravating activities.
Although recovery time varies among patients, physiotherapy for about four to six weeks is usually recommended. The aim of our treatment is to calm pain and inflammation, to correct muscle imbalances, and to improve the function of the quadriceps mechanism.
With the The Cambridge Physiotherapy rehabilitation program, many patients are able to return to their previous level of activity without recurring symptoms.
Post-surgical Rehabilitation
Many surgeons will have their patients take part in formal physiotherapy after knee surgery for patellofemoral problems. More involved surgeries for patellar realignment or restorative procedures for tendon tissue require a delay before going to therapy. Rehabilitation may be slower to allow the tendon to heal before too much strain can be put on the knee.
When you begin your physiotherapy program, treatments are designed to help control the pain and swelling from the surgery. Our physiotherapist will choose exercises to help improve knee motion and to get the quadriceps muscles toned and active again. Muscle stimulation, using electrodes over the quadriceps muscle, may be needed at first to get the muscle moving again.
As your program evolves, more challenging exercises are chosen to safely advance the knee's strength and function. The key is to get the soft tissues in balance through safe stretching and gradual strengthening.
At The Cambridge Physiotherapy our goal is to help you keep your pain under control, ensure you place only a safe amount of weight on the healing knee, and improve your strength and range of motion. When your recovery is well under way, regular visits to our office will end. Although we will continue to be a resource, you will be in charge of doing your exercises as part of an ongoing home program.
The Cambridge Physiotherapy provides services for physiotherapy in Cambridge, Galt, and Preston.
Physician Review
X-rays may be ordered on the initial visit to your doctor. An X-ray can show fractures or the presence of calcium deposits in the quadriceps muscle but X-rays do not show soft tissue injuries. In these cases, other tests, such as ultrasonography or magnetic resonance imaging (MRI), may be suggested. Ultrasound uses sound waves to detect tendon tears. MRIs use magnetic waves rather than X-rays to show the soft tissues of the body. This machine creates pictures that look like slices of the knee. Usually, this test is done to look for injuries, such as tears in the quadriceps. This test does not require any needles or special dye and is painless.
Surgery
Surgery is rarely needed when a wide range of protective measures, relative rest, ice, support, and rehab are used. If nonsurgical treatment fails to improve your condition, then surgery may be suggested. Surgery is designed to stimulate healing through revascularization (restoring blood supply). Weak, damaged tissue is removed and the injured tendon is repaired. Tissue remodeling through surgery can restore function.
Arthroscopic procedures can usually be done on an outpatient basis. This means you can leave the hospital the same day. If your problem requires a more involved surgical procedure where bone must be cut to allow moving the quadriceps tendon attachment, you may need to spend one or two nights in the hospital.
Portions of this document copyright MMG, LLC.









