Introduction
Physiotherapy in Cambridge, Galt, and Preston for Wrist
Welcome to The Cambridge Physiotherapy's patient resource about de Quervain's Tenosynovitis.
The condition called de Quervain's tenosynovitis causes pain on the inside of the wrist and forearm just above the thumb. It is a common problem affecting the wrist and is usually easy to diagnose.
This guide will help you understand:
- how this condition starts
- how to recognize the symptoms
- what can be done to stop the pain
#testimonialslist|kind:all|display:slider|orderby:type|filter_utags_names:Hand Pain|limit:15|heading:Hear from some of our patients who we treated for *Hand Pain*#
Anatomy
What part of my thumb and wrist is causing problems?
De Quervain's tenosynovitis affects . These tendons are called the abductor pollicis longus (APL) and the extensor pollicis brevis (EPB).
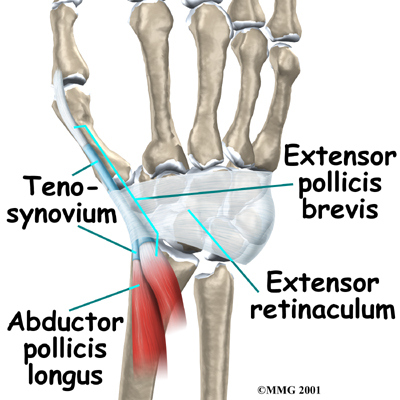
Tendons connect muscle to bone. Muscles pull on tendons for movement. The
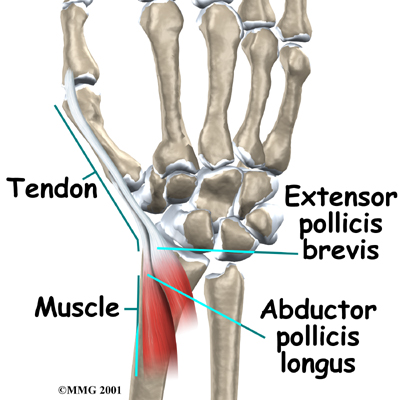
to the APL and EPB tendons are on the back of the forearm. The muscles angle toward the thumb.
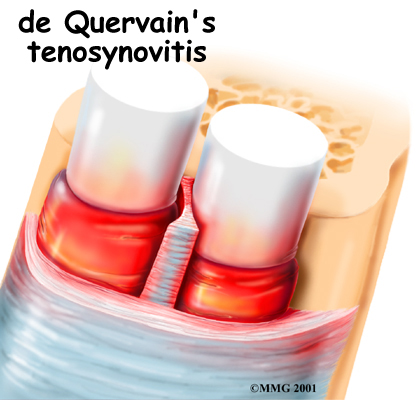
On their way to the thumb, the APL and EPB tendons travel side by side along the inside edge of the wrist. They pass through a
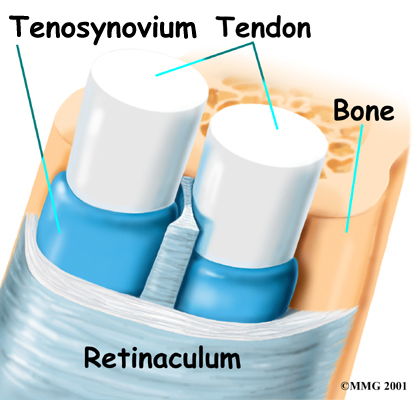
near the end of the radiusbone of the forearm. The tunnel helps hold the tendons in place, like the guide on a fishing pole.
This tunnel is lined with a slippery coating called tenosynovium. The tenosynovium is a slippery covering that allows the two tendons to glide easily back and forth as they move the thumb. Inflammation of the tenosynovium and tendon is called tenosynovitis. In de Quervain's tenosynovitis, the inflammation constricts the movement of the tendons within the tunnel.
Related Document: The Cambridge Physiotherapy's Guide to Wrist Anatomy
Causes
How did this condition develop?
Repeatedly performing hand and thumb motions such as grasping, pinching, squeezing, or wringing may lead to the inflammation of tenosynovitis. This inflammation can lead to swelling, which hampers the smooth gliding action of the tendons within the tunnel. Arthritic diseases that affect the whole body, such as rheumatoid arthritis, can also cause tenosynovitis in the thumb. In other cases, scar tissue from an injury can make it difficult for the tendons to slide easily through the tunnel.
Symptoms
What problems does this condition cause?
At first, the only sign of trouble may be soreness on the thumb side of the forearm, near the wrist. If the problem isn't treated, pain may spread up the forearm or further down into the wrist and thumb.
As the friction increases, the two tendons may actually begin to squeak as they move through the constricted tunnel. This noise is called crepitus. If the condition is especially bad, there may be swelling along the tunnel near the edge of the wrist. Grasping objects with the thumb and hand may become increasingly painful.
Diagnosis
How will my health care provider identify my problem?
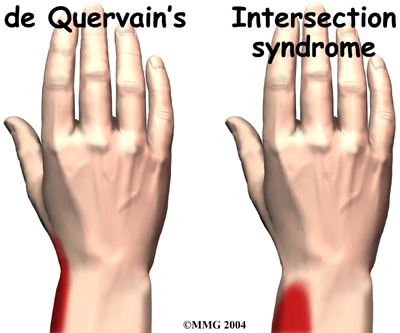
When you visit The Cambridge Physiotherapy, we usually diagnose de Quervain's tenosynovitis easily through a physical examination. Most of the time no special tests are required. The major problem can be distinguishing de Quervain's tenosynovitis from intersection syndrome, which is a very similar condition.
Careful attention must be paid to where the pain is located: over the de Quervain's tunnel near the end of the radius bone, or over the intersection point on the wrist. The intersection point is about three inches up the forearm.
The Finklestein test is one of the best ways to make the diagnosis. You can do this test yourself. Bend your thumb into the palm and grasp the thumb with your fingers making a fist with the thumb inside. Now bend your wrist away from your thumb. If you feel pain over the tendons to the thumb, your problem may be de Quervain's tenosynovitis.
Once your diagnostic examination is complete, the physiotherapists at The Cambridge Physiotherapy have treatment options that will help speed your recovery, so that you can more quickly return to your active lifestyle.
Our Treatment
Non-surgical Rehabilitation
If at all possible, you must change or stop all activities that cause your symptoms. Take frequent breaks when doing repeated hand and thumb actions. Avoid repetitive hand motions such as heavy grasping, wringing, or turning and twisting movements of the wrist. Keep the wrist in a neutral alignment. In other words, keep it in a straight line with your arm, without bending it forward or backward.
 After your injury is evaluated, our physiotherapist may want you to wear a special forearm and thumb splint called a . This splint keeps the wrist and lower joints of the thumb from moving. The splint allows the APL and EPB tendons to rest, giving them a chance to begin to heal.
After your injury is evaluated, our physiotherapist may want you to wear a special forearm and thumb splint called a . This splint keeps the wrist and lower joints of the thumb from moving. The splint allows the APL and EPB tendons to rest, giving them a chance to begin to heal.
Anti-inflammatory medications may also help control the swelling of the tenosynovium and ease symptoms. These medications include common over-the-counter medications such as ibuprofen and aspirin.
When you begin your The Cambridge Physiotherapy program, the main focus of our physiotherapy is to reduce or eliminate the cause of irritation of the thumb tendons. Our physiotherapist may check your workstation and the way you do your work tasks. We may provide suggestions about the use of healthy body alignment and wrist positions, helpful exercises, and tips on how to prevent future problems.
If nonsurgical treatment is successful, you may see improvement in about four to six weeks. You may need to continue wearing your thumb splint to control symptoms. Try to do your activities using healthy body and wrist alignment, and limit activities that require repeated motions of the wrist and thumb.
Post-surgical Rehabilitation
Rehabilitation is more involved after surgery. Full recovery could take several months. Pain and symptoms generally begin to improve after surgery, but you may have tenderness in the area of the incision for several months.
Take time during the day to support your arm with your hand elevated above the level of your heart. You should move your fingers and thumb occasionally during the day. Keep the dressing on your hand until you return to the surgeon. Avoid getting the stitches wet. Your stitches will be removed 10 to 14 days after surgery.
Although the time required for recovery is different for each patient, as a general rule, you will probably need to attend your physiotherapy sessions for six to eight weeks. Our therapist will have you begin by doing active hand movements and range-of-motion exercises. We may also use ice packs, soft-tissue massage, and hands-on stretching to help with the range of motion.
When the stitches are removed, you may start carefully strengthening your hand and thumb by squeezing and stretching putty. Our physiotherapists also use a series of gentle stretches to encourage the thumb tendons to glide easily within the tunnel.
As you progress, our physiotherapist will give you exercises to help strengthen and stabilize the muscles and joints in your hand and thumb. We may also use other exercises to improve fine motor control and dexterity. Some of the exercises we’ll recommend are designed to get your hand working in ways that are similar to your work tasks and sport activities.
Our physiotherapist will help you find ways to do your tasks that don't put too much stress on your thumb and wrist. Before your physiotherapy sessions end, our physiotherapist will teach you a number of ways to avoid future problems.
The Cambridge Physiotherapy provides services for physiotherapy in Cambridge, Galt, and Preston.
Physician Review
Your doctor may suggest an injection of cortisone into the irritated tunnel. Cortisone reduces the swelling of the tenosynovium and may temporarily relieve your symptoms. Cortisone injections will usually control the inflammation in the early stages of the problem.
Surgery
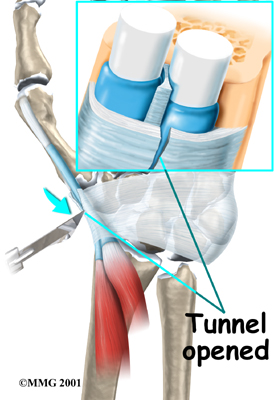
If all else fails, you may need surgery. The goal of surgery is to give the tendons more space so they no longer rub on the inside of the tunnel. To do this, the surgeon performs a surgical release of the roof of the tunnel.
This surgery can usually be done on an outpatient basis, which means that you won't have to spend the night in the hospital. It can be done using a general anesthetic, which puts you to sleep, or a regional anesthetic. A regional anesthetic blocks the nerves going to only a certain part of the body. Injection of medications similar to novocaine can block the nerves for several hours.
In surgery for de Quervain's tenosynovitis, you may get an axillary block, which puts the arm to sleep, or a wrist block, which puts only the hand to sleep. It is even possible to perform the surgery by simply injecting novocaine around the area of the incision.
Once you have anesthesia, your surgeon will make sure the skin of your forearm and wrist is free of infection by cleaning the skin with a germ-killing solution. The first step in the surgical release is to make a along the thumb side of the wrist.

The surgeon moves aside other tissues and locates the tendons and the tunnel. An . This allows the tunnel to open up, creating more space for the tendons. The tunnel will eventually heal closed, but it will be larger than before. Scar tissue will fill the gap where the tunnel was cut.
The skin is then stitched together, and your hand is wrapped in a bulky dressing.
Portions of this document copyright MMG, LLC.









